
Carbon monoxide exposed patients commonly present with nonspecific symptoms that mimic influenza-like illnesses (Table 1). Symptoms typically include headache, dizziness, nausea, vomting, weakness, and fatigue. The most common symptom reports is headache.
Our friends and colleagues at the Undersea and Hyperbaric Medical Society (UHMS) invite you to enjoy a complimentary copy of Pressure, the Society's bimonthly newsletter. |
5256 Hits
Photo Caption: The decompression chamber aboard the USS Dixon where David Scalia suffered his third cardio-respiratory arrest. Dr. Greg Adkission successfully resuscitated David and remained with him in the chamber for 12 hours.
7263 Hits
More than 100 years ago, Sorbonne Professor Paul Bert, the father of pressure physiology, explained, “All symptoms, from the slightest to those that bring on sudden death, are the consequences of the liberation of bubbles of nitrogen in the blood [on-gassing], and even in the tissues, when compression has lasted long enough. The great protection is slowness of decompression [off-gassing].”
9764 Hits
In 1982, when David Scalia was evacuated to San Diego after suffering an air embolism to his brain, there was no hyperbaric chamber in the city.
6508 Hits
A textbook may sometimes gain the unusual trait of longevity beyond all other books — it can be revised
and remain a primary source of information for generations of students.
7640 Hits
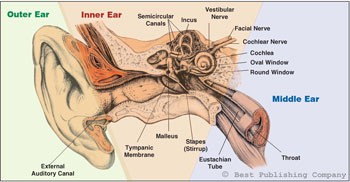
Sinus and internal and external ear disorders are the most common side effects of hyperbaric oxygen therapy (HBO2).1 These spaces are the cranium’s pneumatic sockets and, particularly those of the middle and inner ear, are most frequently involved in the pressure stress caused by compression and decompression maneuvers during exposure to altered pressures in the hyperbaric chamber. Barotrauma is the mechanical tissue damage produced by environmental pressure variation, and the middle ear is the most frequently involved structure in this kind of damage. According to Boyle’s law (the product of pressure and volume is a constant for a given mass of confined gas) it is easy to understand why all enclosed air cavities are more susceptible to this kind of lesion. Barotraumas can occur due to an increase or decrease of gas volume. To avoid gas volume decrease during the compression phase, the patient must perform some compensatory maneuvers aimed at inhaling and forcing gas (air or oxygen) into the nasal and sinus cavities. During decompression in the chamber or even underwater, the body’s gas expands and is expelled from cavities to the outside, usually without any active maneuver. It is essential to teach the patient about the functions of the hyperbaric chamber and the correct maneuvers of baro compensation. In this article, we will describe the main barotraumas that can occur during hyperbaric oxygen therapy.
Copyright
© Best Publishing Company. This article first appeared in Wound Care & Hyperbaric Medicine Magazine Vol 6 Issue 1 (Spring), 2015.
48903 Hits
February is Heart Month and to support the movement we have teamed up with our sister company, Wound Care Education Partners, to bring you valuable resources and discounts. We invite you to learn more about cardiac issues as related to hyperbaric and undersea medicine and take advantage of these free and discounted resources on the topic.
12488 Hits